Metastatic Esophageal Cancer
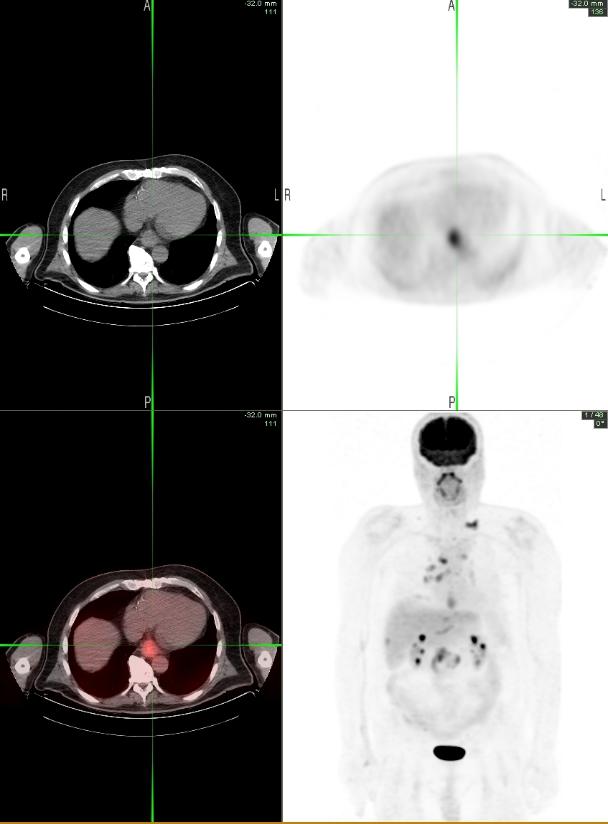
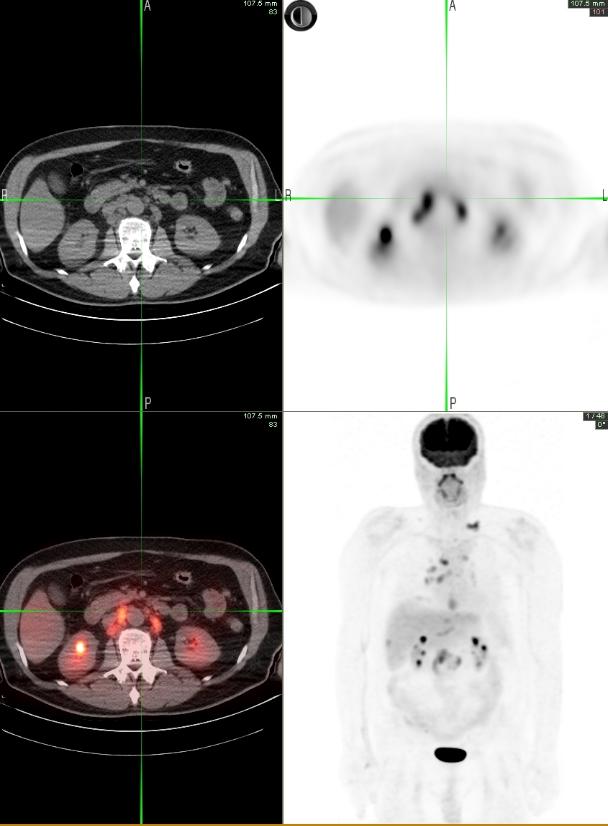
A 63 years old male with past medical history of CABG presented with a 2-3 week history of dysphagia. He was able to localize a point in the region of his distal esophagus where solid foods were getting ‘stuck.’ He was able to drink some liquids but noted that they too were passing with increasing difficulty. An EGD was performed by GI and a circumferential mass was seen at the lower end of esophagus. Biopsy showed invasive moderately differentiated adenocarcinoma. CT scan showed the mass at the distal esophagus, and lymphadenopathy in the aorto-pulmonary window, adjacent to the celiac trunk and along the lesser curvature of the stomach. EUS could not be performed due to luminal narrowing. A whole body PET-CT was acquired for initial staging and to evaluate for distant metastasis.
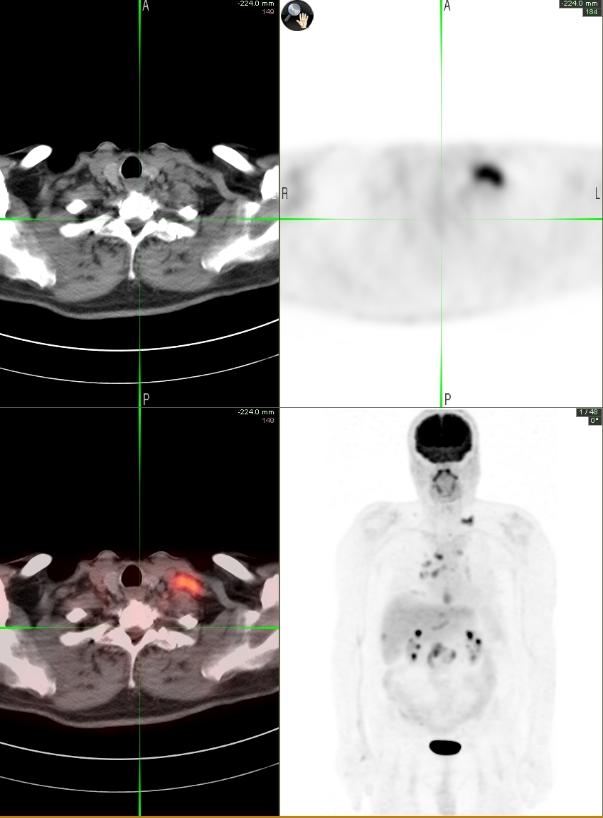
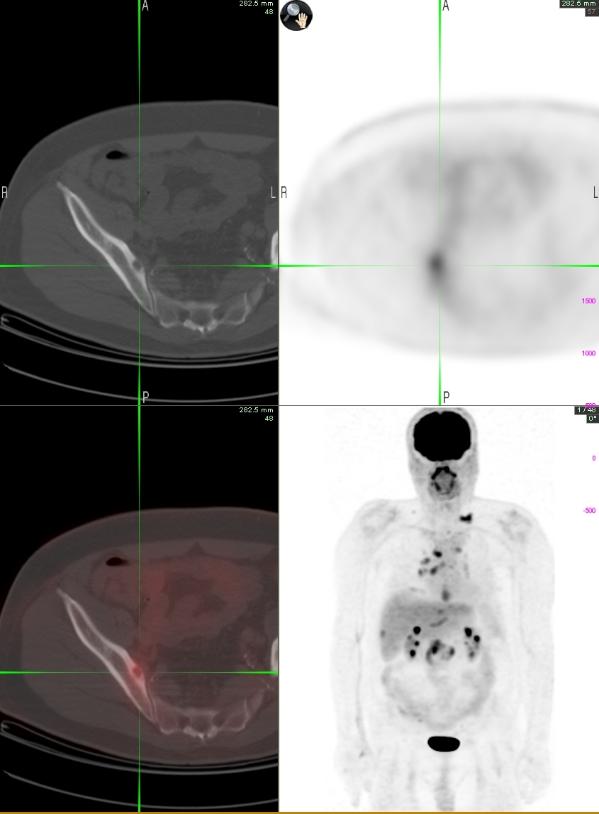
PET-CT images show a hypermetabolic lesion in the distal esophagus consistent with malignancy. Hypermetabolic lymphadenopathy (max SUV 8.3) is seen in the abdomen and thorax, and also in the left supraclavicular region (Virchow’s node), consistent with metastasis. Multiple small hypermetabolic lesions are seen in the liver, suspicious for metastasis. A hypermetabolic and lytic lesion seen in the right ilium, and focal uptake seen in the left pedicle of T3 are consistent with bone metastasis.
1. The evolving role of PET-CT in the management of esophageal cancer. Chuang HH, Macapinlac HA. Q J Nucl Med Mol Imaging. 2009 Apr;53(2):201-9.
2. The role of 18F-FDG PET/CT in the evaluation of oesophageal carcinoma. Chowdhury FU, Bradley KM, Gleeson FV. Clin Radiol. 2008 Dec;63(12):1297-309.
This case was compiled by Dr. Sania Rahim-Gilani, BCM