Category
Gnuc-com
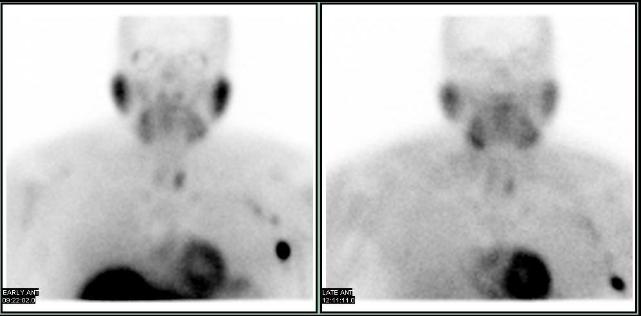
Hepatic Hydrothorax on Peritoneal Scintigraphy
Dr. Kallel Faouzi, Consultant in Nuclear Medicine, King Faisal Hospital, Taif-Saudi Arabia
A 78-year-old female with cirrhosis presented with ascites and persistent right-sided pleural effusion. Hepatic hydrothorax was suspected, and peritoneal scintigraphy was performed after intraperitoneal injection of 259 MBq of 99mTc-nano colloids. Dynamic early and static images centered on the thorax and abdomen were acquired at 1, 1:30, and 2 hours post-injection.
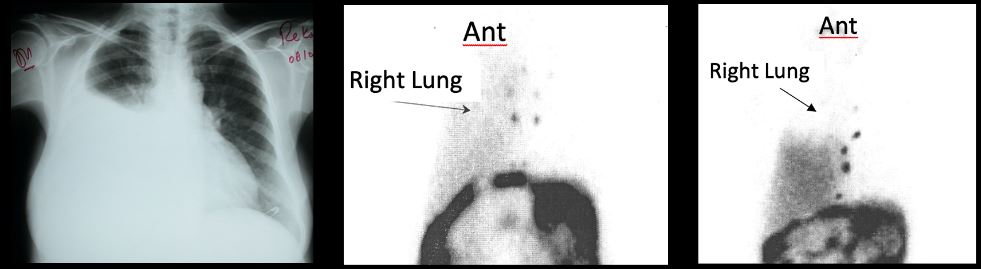
Progressive accumulation of the radio-pharmaceutical in the right pleural space (seen above on 1 hr and 2 hr images), in the pattern of known pleural effusion, is consistent with hepatic hydrothorax. The patient was treated successfully with talc pleurodesis.
Ajmi S, Hassine H, Guezguez M, Elajmi S, Mrad Dali K, Karmani M, Zayane A, Essabbah H. Isotopic exploration of hepatic hydrothorax: ten cases, Gastroenterol Clin Biol. 2004 May;28(5);462-6.
Mittal BR, Maini A, Das BK. Peritoneopleural communication associated with cirrhotic ascites: scintigraphic demonstration. Abdom Imaging. 1996 Jan-Feb;21(1):69-70.
Gastric Emptying in Situs Inversus
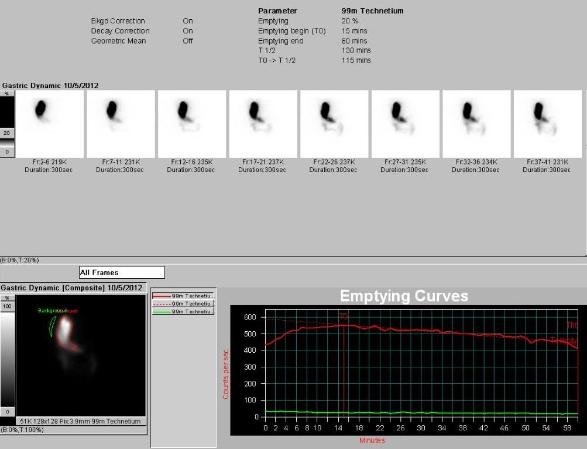
Patient is a 27 -year-old male with history of lung transplant who was referred for gastric emptying study, to evaluate for gastroparesis. Dynamic images of the stomach were acquired 1 minute per frame for 1 hr, in anterior and posterior projections, after the oral administration of an egg sandwich labeled with approximately 1.0 mCi of Tc-99m sulfur colloid.
The dynamic images above show a reversed contour of the stomach. The protocol displays images from the anterior camera head first, followed by the posterior camera head. Camera head positioning was confirmed and patient’s history reviewed. The ROI analysis below shows gastroparesis with only 20% emptying at the end of 1 hour.
Situs inversus is a congenital condition in which transposition of the viscera in the thorax and abdomen occurs where the major visceral organs are reversed or mirrored from their normal positions. The heart is located on the right side of the thorax, the stomach and spleen on the right side of the abdomen and the liver and gall bladder on the left side.
Approximately 25% of patients with complete situs inversus also have Primary Ciliary Dyskinesia (Kartagener Syndrome), characterized by the triad of situs inversus, chronic sinusitis, and bronchiectasis.
Representative images from patient’s CT scan confirm Situs Inversus and location of the fundus of the stomach, below the right hemi-diaphragm.

Post Therapy Scans
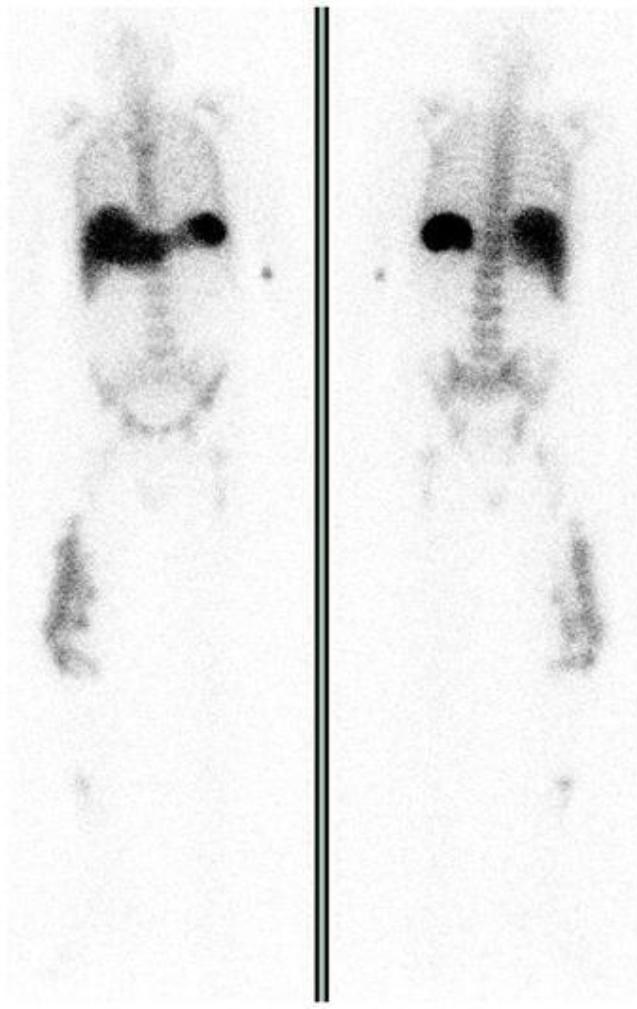
Patient is a 57 -year-old female with history of pancreatic neuroendocrine cancer and distal pancreatectomy 12 yrs ago. She developed liver metastases and underwent liver transplant about 7 yrs ago. She has received multiple cycles of chemotherapy for metastatic abdominal lymphadenopathy and presents with progressive disease and multiple bilateral lung nodules.
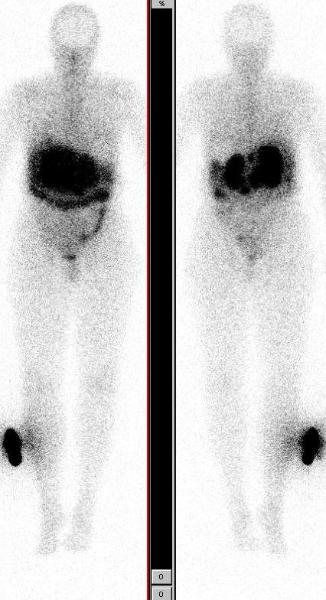
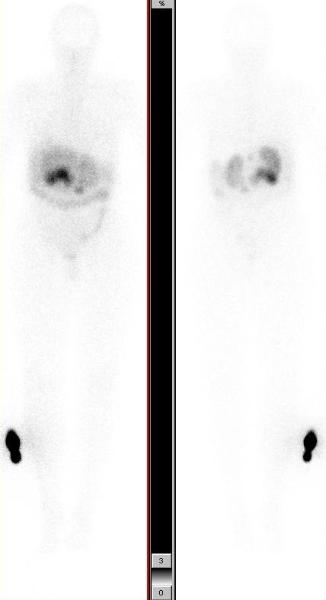
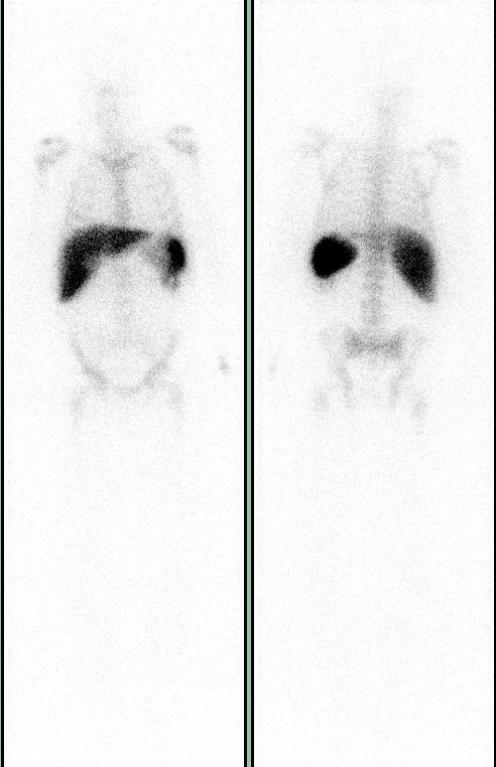
Images above show In-111 Octreotide scan in anterior and posterior projections, in dark and light intensities showing focal uptake in abdominal lymphadenopathy. She is asymptomatic, her Karnofsky performance score is 100 and the neuroendocrine markers not elevated.
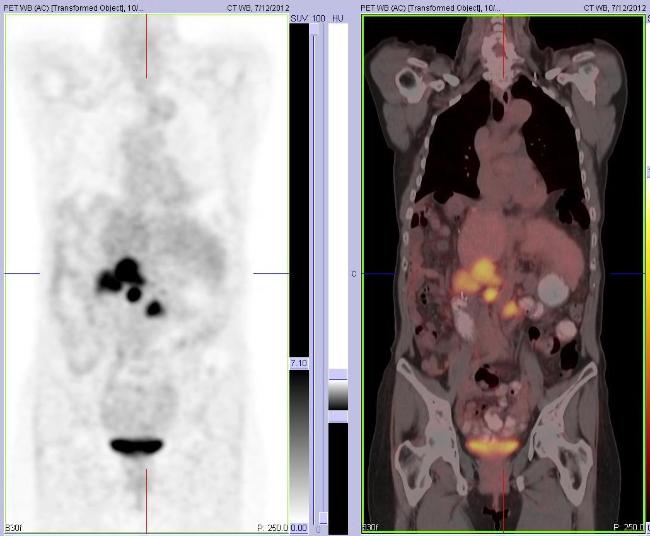
The whole body FDG PET/CT scan shows focal hypermetabolism in abdominal lymphadenopathy and mild uptake in bilateral lung nodules. She met the inclusion and exclusion criteria for investigational PRRT (Peptide Receptor Radionuclide Therapy) with high dose In-111 Octreotide and was enrolled in the protocol.
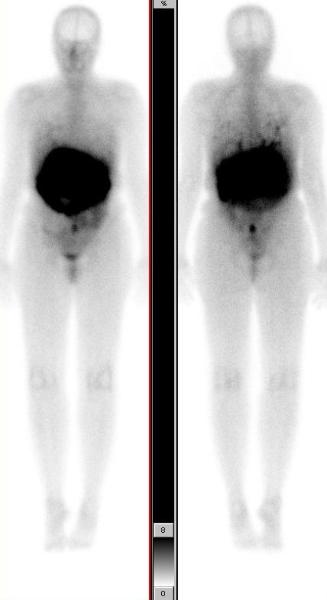
Images below show post therapy scans acquired 48 hrs after PRRT with 471.0 mCis of In-111 Octreotide. The anterior and posterior whole body scans are presented in two different intensities. They show good targeting with intense uptake in metastatic lymphadenopathy and uptake in bilateral lung nodules (scan shown in higher intensity).
This case illustrates the role of post therapy scan in confirming the metastatic etiology of bilateral lung nodules. These nodules did not show any uptake with the low dose of In-111 Octreotide used for diagnostic imaging, but were seen to take up In-111 Octreotide on the post therapy scan. This is likely due to higher radiopharmaceutical activity used for therapy, as compared to the diagnostic scan. This phenomenon is frequently seen in treatment of thyroid cancer patients with I-131, and comparing the I-131 post therapy scan with the diagnostic low dose I-131 scan.

Is detection of additional lesions in post-peptide receptor radionuclide therapy scans with respect to diagnostic imaging only due to different affinity of ligands?: a report of discordance between diagnostic and posttherapy imaging using the same ligand. Minutoli F, Herberg A, Sindoni A, Cardile D, Cucinotta M, Baldari S. Clin Nucl Med. 2012 Aug;37(8):817-8.
Dislocated Hip Prosthesis
An 86 years old female with bilateral hip prosthesis presented with pain in the left lower extremity, radiating to the upper and medial thigh. The pain is worse with activity and is relieved with rest. No history of injury. Past medical history is significant for high blood pressure, high cholesterol, cerebrovascular accident, and osteoporosis. The left hip prosthesis has been revised several times in the past. Patient complains of pain with resisted flexion of left hip. There is no evidence of swelling or skin lesions. X ray of the left hip shows possible loosening and subluxation. A three phase bone scan was performed.
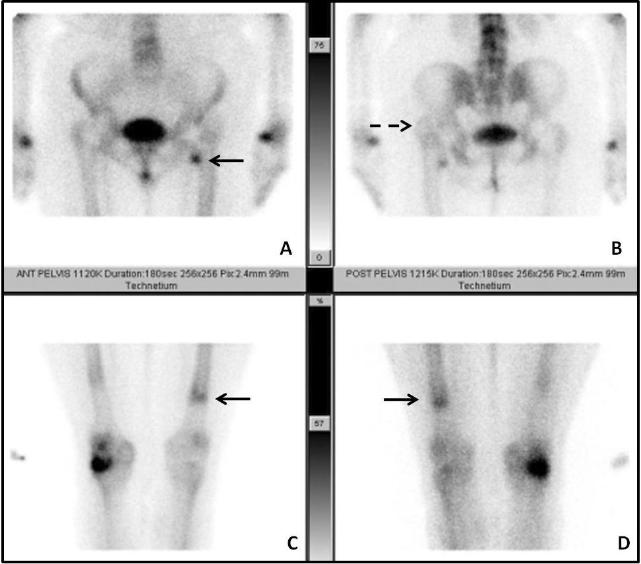
Blood flow and blood pool images (not shown) were significant for mild focal hyperemia in the left lesser trocanter. The delayed images show several signs of prosthesis dislocation. The head of the prosthesis is located in the acetabulum, but the femur has dislocated posteriorly and superiorly relative to the prosthesis.
Image A shows focal uptake in the left lesser trocanter, suspicious for fracture. Image B shows superior location of the left greater trocanter relative to the right hip. Images C & D show focal uptake at the distal end of the prosthesis from the downward dislocation of the prosthesis, relative to the femur.
Three phase bone scan is the standard of care for patients presenting with symptoms and sign suggestive of prosthesis complication. It is usually followed up with an In-111 WBC scan to evaluate for infection and sometimes with a third sulfur colloid bone marrow scan to confirm or rule out active infection.
Nuclear medicine and the infected joint replacement. Love C, Marwin SE, Palestro CJ. Semin Nucl Med. 2009 Jan;39(1):66-78.
This case was compiled by Dr. Amin Samarghandi, Excel Diagnostics
Cerebrospinal Fluid Leak
A 41 year old Caucasian male with a history of hypertension presented to the emergency room with a 3 week history of worsening headache and neck stiffness. His neurologic exam was unremarkable for focal deficits. CT scan and MRI showed bilateral subdural collections suggesting chronic subdural hematomas due to intracranial hypotension. Radionuclide cisternography was performed with intra-thecal injection of In-111 DTPA through lumbar puncture, followed by planar imaging at 2 and 24 hrs and SPECT/CT imaging at 24 hrs.
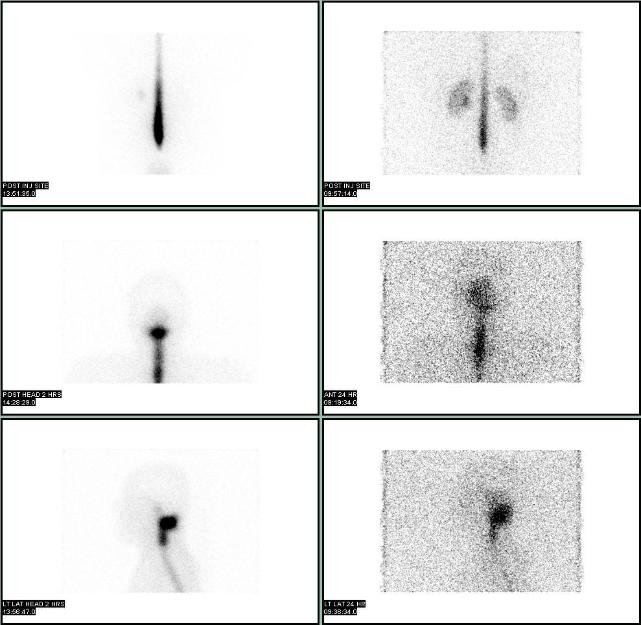
An abnormal focus of intense uptake was seen at the base of the skull on 2 hr and 24 hr planar images, without any discernable basal cistern or lateral ventricle activity or activity around the convexities. SPECT/CT localized the CSF leak to outside the thecal sac in the soft tissues between C1 and C2 towards the left of the midline. Subsequent MRI of the cervical spine confirmed the location and extent of CSF leak. After the placement of epidural blood path, patient reported dramatic improvement of his headaches.
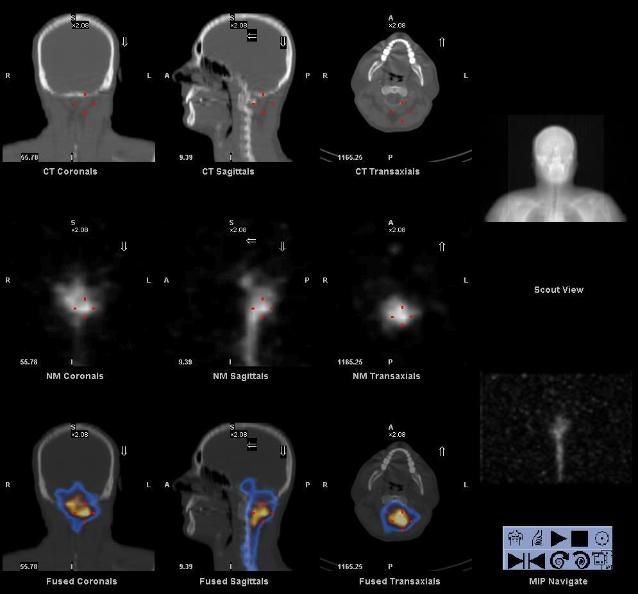

Radionuclide cisternography is a very sensitive for the detection of CSF leak. Once CSF leak is identified on planar images, SPECT/CT can be performed to localize the site and visualize other pathology.
This case was compiled by Dr. David He, BCM
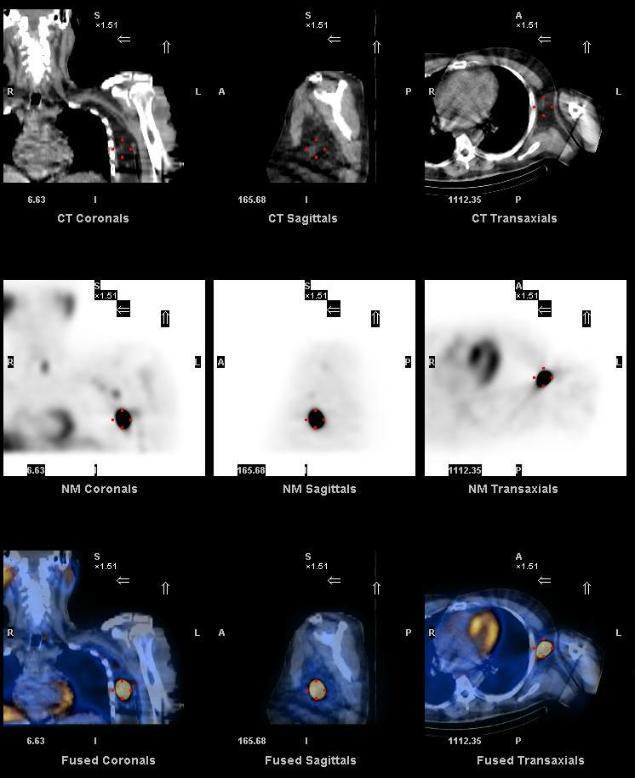
Prosthesis Related Abscess
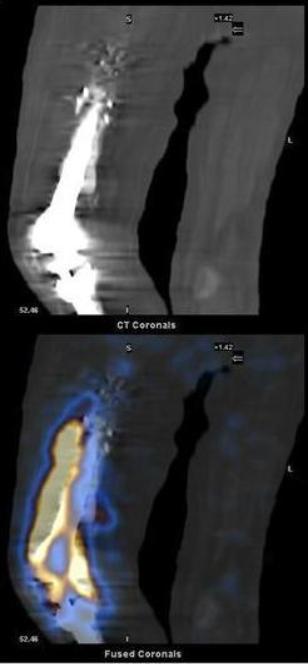
A 77-year-old male with history of right knee joint replacement 4 years ago, presented with swelling and pain following a fall. He soon developed fever with elevated WBC count, ESR and CRP. Blood cultures were negative. Whole body images were acquired in anterior and posterior projections, after the intravenous administration of 543 μCi of In-111 labeled autologous WBCs. They show a large area of abnormal accumulation of labeled WBCs in right thigh.
CT and fused SPECT/CT images in the coronal plane localize the uptake to the antero-lateral aspect of the right femoral prosthesis, extending into the knee.
Transaxial CT and fused SPECT/CT images localize the uptake to an abnormal density with an air fluid level, characteristic of an abscess. Patient underwent drainage, irrigation and debridement.
In-111 labeled leukocyte scintigraphy is the imaging modality of choice for evaluation of patients with suspected joint replacement infections. As compared to CT and MRI, scintigraphy is not limited by orthopedic hardware, and in combination with bone marrow scan (using Tc-99m sulfur colloid), provides excellent sensitivity and specificity in the diagnosis of prosthesis infection.
SPECT/CT is gaining popularity as a hybrid imaging modality where the functional (scintigraphic) and anatomic (low dose CT) information is acquired together to generate coregistered images. SPECT/CT imaging has been shown to improve sensitivity and specificity of labeled leukocyte imaging by providing precise localization and extent of abnormalities. This case highlights the importance of SPECT/CT hybrid imaging in In-111 leukocyte scintigraphy.
1. Love C, Marwin SE, Palestro CJ. Nuclear medicine and the infected joint replacement. Semin Nucl Med 2009;39:66-78.
2. Mulamba L, Ferrant A, Leners N, de Nayer P, Rombouts JJ, Vincent A. Indium-111 leucocyte scanning in the evaluation of painful hip arthroplasty. Acta Orthop Scand 1983;54:695-7.
3. Palestro CJ, Swyer AJ, Kim CK, Goldsmith SJ. Infected knee prosthesis: diagnosis with In-111 leukocyte, Tc-99m sulfur colloid, and Tc-99m MDP imaging. Radiology 1991;179:645-8.
4. Bar-Shalom R, Yefremov N, Guralnik L, Keidar Z, Engel A, Nitecki S, Israel O. SPECT/CT using 67Ga and 111In-labeled leukocyte scintigraphy for diagnosis of infection. J Nucl Med 2006;47:587-94.
5. Filippi L, Schillaci O. Usefulness of hybrid SPECT/CT in 99mTc-HMPAO-labeled leukocyte scintigraphy for bone and joint infections. J Nucl Med 2006;47:1908-13.
This case was compiled by Dr. Farbod Nasseri, BCM
Abdominal Abscess
A 54 year old male with a history of hepatitis C, stage II colon cancer, status post left hemicolectomy presented for follow-up of a newly diagnosed left tonsillar squamous cell carcinoma. A whole body FDG PET/CT was preformed for staging, two months after the surgery for colon cancer. Focal hypermetabolism was seen in the left tonsillar mass and left level II lymphadenopathy. Incidentally noted increased uptake in the left upper quadrant of the abdomen was thought to be related to post surgical changes at the site of prior bowel anastomosis. Patient also has history of recurrent MRSA infections (subcutaneous abscess in the lower extremity, groin, and axilla).
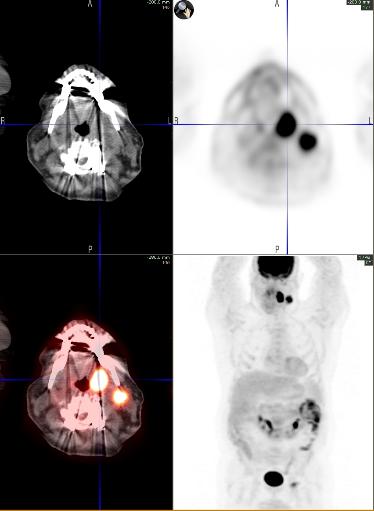
Soon after initiating chemotherapy patient was admitted for fever with chills and was found to have MRSA bacteremia. In-111 labeled leukocyte (WBC scan) study was performed with 657 microcuries to identify the source of infection. Planar images show ill defined focal uptake in the left upper quadrant of the abdomen, abutting the spleen.
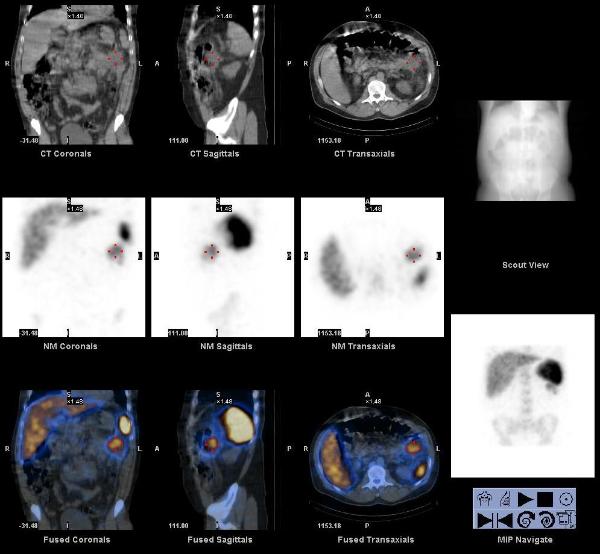

The SPECT/CT images localize the focus to the splenic flexure of colon, at the site of prior bowel anastomosis, post left hemicolectomy. This abnormal accumulation of In-111 labeled WBCs was suspicious for active infection. A follow up contrast enhanced CT scan of the abdomen showed an abscess in this region, that was drained.
Early investigation of hybrid SPECT/CT imaging technology in localizing infection has been very promising. This could lead to a greater acceptance of this technology in a wide variety of additional clinical roles as well.
Bybel, B et al. SPECT/CT imaging: clinical utility of an emerging technology. Radiographics. 2008 Jul-Aug;28(4):1097-1113.
Heiba, S et al. The diagnostic confidence of SPECT & SPECT/CT in Indium-111 leukocyte scintigraphy. J Nucl Med. 2007; 48 (Supplement 2):63P.
This case was prepared by Dr. Raj R Chinnappan BCM
Diabetic Foot Infection
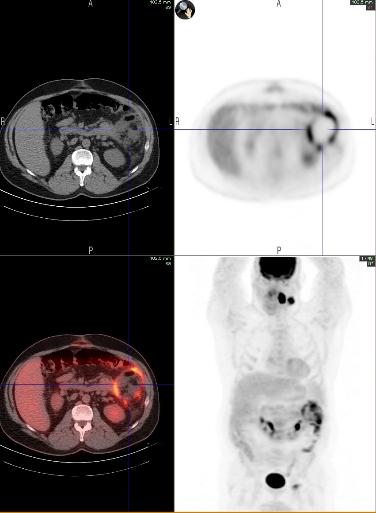
A 75 year old male with a history of type II diabetes mellitus presented for further evaluation of an ulcer on the distal lateral aspect of the right foot. It had worsened with conservative treatment in the last few months with symptoms of swelling, tenderness, and drainage. Underlying osteomyelitis was suspected.
Radiographs of the foot demonstrated midfoot arthrosis and old postsurgical changes from a 4th ray amputation at the level of the distal 4th metatarsal, but no evidence of osteomyelitis.

An In-111 labeled leukocyte study (WBC scan) was performed after the intravenous injection of autologous WBCs labeled with 540 microcuries of In-111. Planar images demonstrated a small focus of mild to moderately increased uptake in the region of the ulcer, suggesting active infection. The planar images lack the anatomical landmarks / resolution to tell whether the uptake is in the soft tissues or bone.
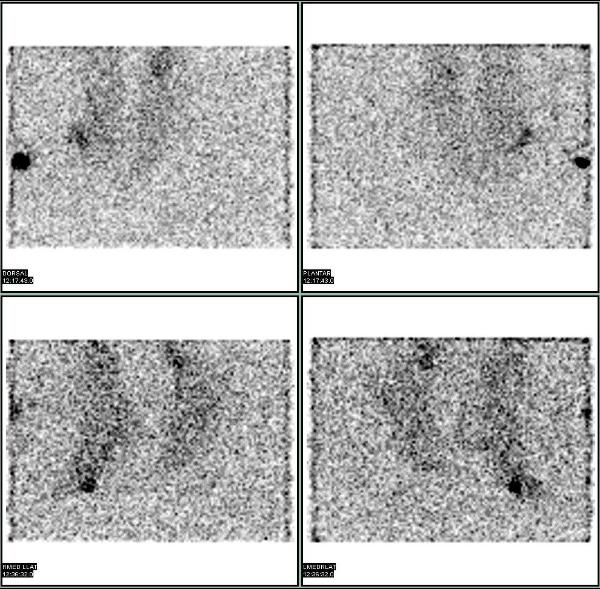
SPECT-CT images of the foot were acquired. The images localize the uptake to the soft tissues and osteomyelitis was ruled out. Fusion of functional SPECT data with structural CT data provides anatomic localization. While this rapidly emerging hybrid imaging technology is of clear benefit in the diagnosis of osteomyelitis in diabetic foot infections, the broader clinical implications from such improved anatomical accuracy are limitless.
Bar-Shalom R, et al. SPECT/CT using 67Ga and 111In-labeled leukocyte scintigraphy for diagnosis of infection. J Nucl Med. 2006 Apr;47(4):587-94.
Horger M, et al. Added value of SPECT/CT in patient suspected of having bone infection: preliminary results. Arch Orthop Trauma Surg. 2007 Apr; 127 (3):211-221.
This case was compiled by Dr. Raj R Chinnappan, BCM
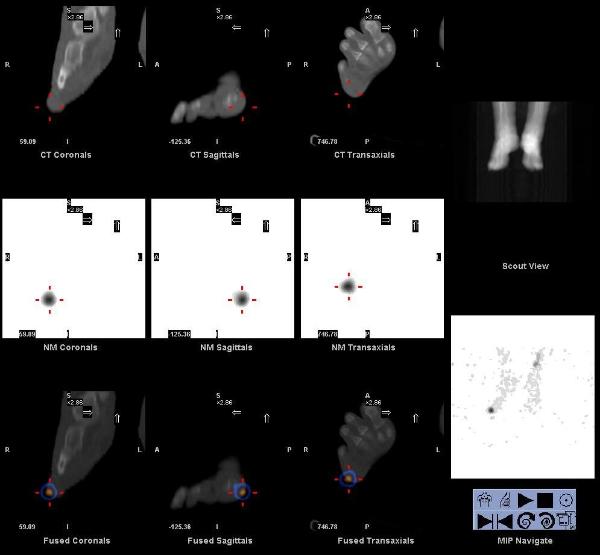
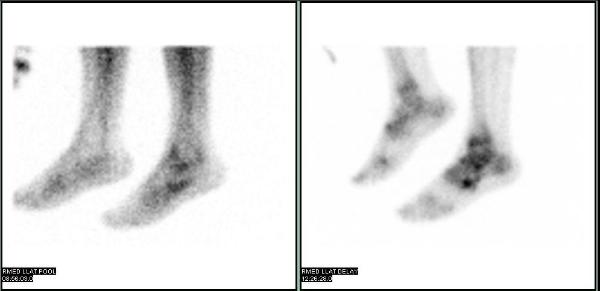
Cuboid Fracture
A 31 year old male presents with left ankle pain and swelling after a twisting injury during a basketball game. The pain radiates down to the anterior lateral proximal foot and is exacerbated when he plays basketball. X-rays of the left tibia/fibula, ankle and foot were unremarkable with no evidence of fracture or dislocation.

A three phase bone scan was performed which showed focal hyperemia on blood flow and blood pool images, and focal osteoblastic activity on the delayed images in the left mid foot. SPECT/CT acquired after the delayed planar images showed that the focal Tc-99m MDP uptake corresponds to a subtle hairline fracture in the cuboid bone (best seen on the saggital projection) on CT images.
Gnanasegaran G et al. Multislice SPECT/CT in Benign and Malignant Bone Disease: When the Ordinary Turns Into the Extraordinary. Seminars in Nuclear Medicine. Volume 39, Issue 6, November 2009, Pages 431-442.
This case was compiled by Dr. Niraj Patel, BCM
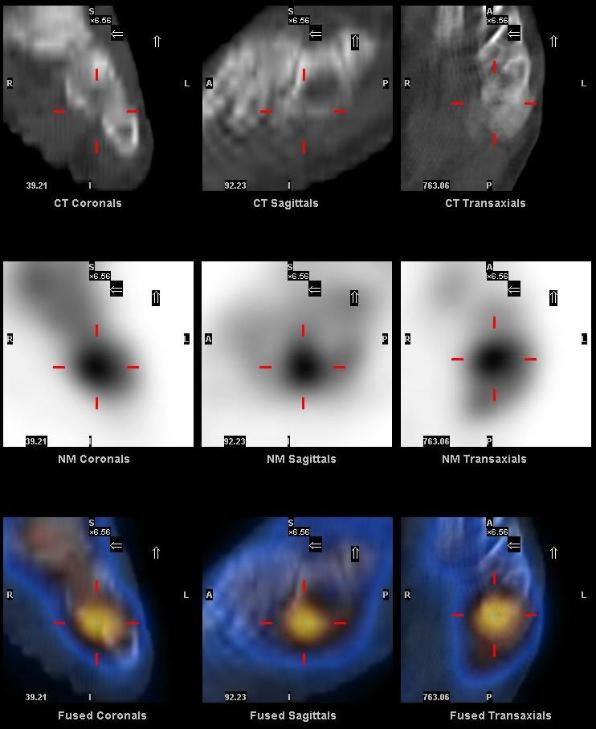
Parathyroid Adenoma
A 70 yrs old male was incidentally found to have hypercalcemia, serum calcium level of 11.9 mg/dl (normal is 8.9 to 10.3). His past medical history included hypothyroidism, prostate carcinoma, atrial fibrillation, type 2 diabetes mellitus, gout, hyperlipidemia, osteoarthritis, migraine and glaucoma. He was found to have an intact PTH level of 373 pg/ml (normal is 16-87) and normal renal function.
Tc-99m Sestimbi scan was performed to localize the probable parathyroid adenoma.
Early and delayed planar images of the neck acquired after intravenous administration of 25.0 mCi of Tc-99m Sestamibi showed a persistent focus of increased uptake at the inferior pole of the left lobe of thyroid, suspicious for a parathyroid adenoma. Focal uptake was also seen in the left axillary and pectoral nodes.
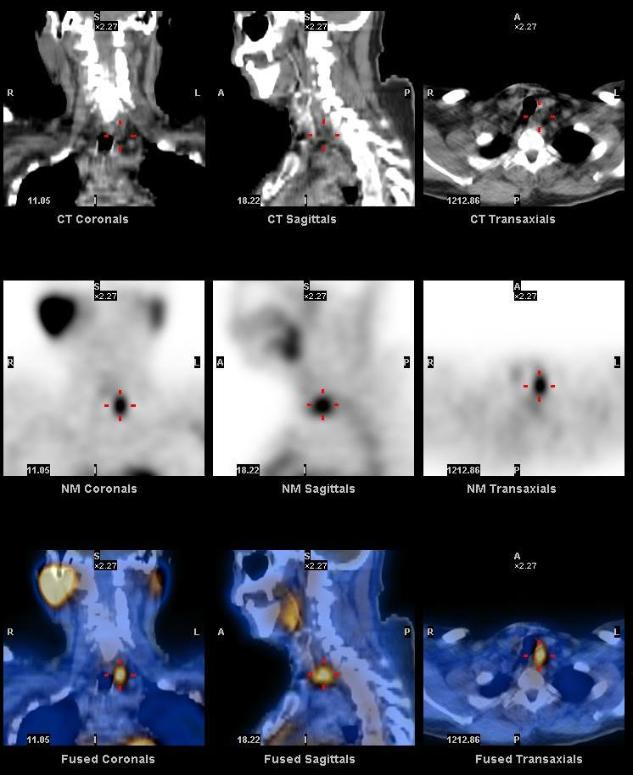
Early SPECT-CT was also acquired and showed the focal abnormal neck uptake to correspond to an abnormal soft tissue density posterior to the left lobe of thyroid. A 1.5 cm parathyroid adenoma was removed from this region at surgery and the intact PTH level dropped to 29 pg/ml.
The axillary uptake corresponded to normal left axillary lymph nodes and felt to be physiologic (secondary to dose inflitration and lymphatic migration) as the tracer was injected in the left antecubital vein.
1. Comparison of SPECT/CT, SPECT, and planar imaging with single- and dual-phase (99m)Tc-sestamibi parathyroid scintigraphy. Lavely WC, Goetze S, Friedman KP, Leal JP, Zhang Z, Garret-Mayer E, Dackiw AP, Tufano RP, Zeiger MA, Ziessman HA. J Nucl Med. 2007 Jul;48(7):1084-9.
2. The value of 99mTc-sestamibi SPECT/CT over conventional SPECT in the evaluation of parathyroid adenomas or hyperplasia. Gayed IW, Kim EE, Broussard WF, Evans D, Lee J, Broemeling LD, Ochoa BB, Moxley DM, Erwin WD, Podoloff DA. J Nucl Med. 2005 Feb;46(2):248-52.
3. Parathyroid scintigraphy in patients with primary hyperparathyroidism: 99mTc sestamibi SPECT and SPECT/CT. Eslamy HK, Ziessman HA. Radiographics. 2008 Sep-Oct;28(5):1461-76.
This case was compiled by Dr. Niraj Patel, BCM